All published articles of this journal are available on ScienceDirect.

A Conceptual-Theoretical-Empirical Structure of Nursing for the Prevention of Delirium Based on the Dynamic Symptom Model
Authors Info & Affiliations
Abstract
Introduction
This study aims to develop a Conceptual-Theoretical-Empirical (C-T-E) structure for holistic nursing care, centered on delirium prevention and treatment in critically ill patients, based on the Dynamic Symptoms Model (DSM) as the theoretical framework.
Methods
The conceptual-theoretical-empirical structure is developed to test theories. The conceptual model or conceptual framework guides the test of the middle-range theory or theoretical framework, linking concepts and propositions. The concepts and propositions are then presented for testing through an empirical research method.
Results
The C-T-E structure, based on the DSM, provides an understanding of delirium as a fluctuating and multifactorial syndrome. Besides, delirium has shown strong associations with physical, psychological, social, environmental, and spiritual antecedents. Thus, nurses and the healthcare team can prevent and reduce delirium in patients by reducing pain, mechanical ventilation, and sedatives, and by managing concomitant symptoms such as anxiety, fear, and suffering, while monitoring the trajectory of delirium. In conclusion, the C-T-E structure of the DSM in the context of delirium provides a theoretical framework for nurses and the healthcare team to personalize holistic, theoretically supported interventions.
Discussion
The practical implications of this study allow us to understand delirium as an event in which various patient antecedents converge. For that, nurses can apply the DSM in nursing interventions to reduce delirium-causing factors in the environment and the patient's antecedents.
Conclusion
This study allows us to understand delirium as an event approach that integrates theory, research, and practice, contributing to delirium prevention and enhancing nursing care quality, expanding inclusive, person-centered healthcare, and reducing the gap between theory, research, and nursing practice, thereby enhancing understanding of the phenomenon.
1. INTRODUCTION
The conceptual-theoretical-empirical (C-T-E) structure is a methodology within nursing knowledge that coherently links theoretical knowledge and nursing practice. The C-T-E structure also supports theory development and theory testing in research [1]. It is therefore a useful tool for bridging the gap between theory, research, and nursing practice [2, 3].
The components of the C-T-E structure are:
- C (Conceptual): conceptual models or theoretical frameworks that orient the disciplinary perspective.
- T (Theoretical): middle-range theories that explain or predict nursing practice phenomena.
- E (Empirical): research tools and methods that allow for the verification of theoretical propositions through observable data [1].
In this way, the C-T-E structure enables the development of nursing interventions grounded in discipline-specific theoretical concepts and aligned with the conceptual model's context. Therefore, the C-T-E is particularly useful for addressing phenomena such as delirium, for which nursing has important implications for prevention and treatment.
Delirium is an acute confusional syndrome that manifests with symptoms such as disorientation, memory loss, psychomotor agitation, hallucinations, and illusions [4-6]. Delirium is associated with both predisposing and precipitating factors. Precipitating factors such as Intensive Care Unit (ICU) stay, pain, noise, artificial light, stress, limited family support, mechanical ventilation, multiple medical devices, and the use of benzodiazepines and opioids may be modifiable through nursing interventions [6, 7]. Delirium is frequent in critically ill patients in intensive care units and can increase the risk of mortality, long hospital stays, and persistent cognitive deficits [4-6].
Despite these consequences, delirium remains underdiagnosed and inadequately managed, often without consideration of precipitating factors, such as environmental adjustments, comfort promotion, family involvement, and maintenance of spatial-temporal orientation [8, 9]. For this reason, nurses can develop interventions to prevent and treat delirium based on disciplinary theories, and focused on modifiable factors, such as comfort promotion, environmental adjustments, family involvement, and maintenance of spatial-temporal orientation [8, 9].
The scientific literature highlights the importance of a nursing theoretical framework that integrates practices focused on modifiable factors within a structured conceptual model aligned with the discipline and a holistic perspective [10]. In this context, the Dynamic Symptoms Model (DSM) proposed by Brant et al. [11, 12] integrates existing theories and models of symptoms and provides an appropriate theoretical foundation for developing nursing interventions for delirium.
The model comprises four fundamental structural elements: Antecedents, Experience and trajectory, interventions, and consequences [11, 12]. Although the model’s application has been partially explored in the literature [13], a systematic translation into a theoretical-empirical structure specifically adapted to nursing practice is still lacking. Therefore, the Dynamic Symptoms Model combined with the C-T-E structure yields a coherent theoretical framework that connects the concepts, propositions, and empirical observations related to delirium. In this perspective, the NNN taxonomy (NANDA-I, NIC, NOC) provides a useful reference for translating theoretical concepts into operational elements, supporting the identification of diagnoses, interventions, and outcomes consistent with the theory. However, this is not the primary objective of this study [14, 15].
Therefore, the research question was: How can the nursing theory, the Dynamic Symptoms Model, guide the design of nursing interventions to prevent and manage delirium in critically ill patients? Hence, the purpose of this work is to develop a Conceptual- Theoretical-Empirical framework based on the Dynamic Symptoms Model to guide the design of nursing interventions to prevent and manage delirium in patients admitted to intensive care units. This integration of theory and practice aims to advance a more coherent, holistic, and discipline-based nursing approach.
2. MATERIALS AND METHODS
The C-T-E structure was developed according to the approaches described by Fawcett [1], specifically for theory development, analysis, and corroboration. The methodological objective was to understand nursing theory and its application in the prevention and treatment of delirium. Thus, a theoretical framework was developed to support the planning of nursing interventions.
The construction of the C-T-E framework was based on a deductive approach, enabling it to link the theoretical concepts of the chosen model with the empirical elements of this phenomenon. The ‘Dynamic Symptom Model’ was chosen as the conceptual model due to its ability to explain the variability, multidimensionality, and interrelationship of its symptoms. These features highlight the complexity of delirium in critically ill patients.
The inquiry included a detailed investigation of the Dynamic Symptoms Model to identify:
- The fundamental concepts that materialize its theoretical schema.
- The underlying assumptions guiding the understanding of the phenomenon, and
- Theoretical propositions explaining connections between the concepts and theoretical features of delirium.
Based on the identified concepts and assumptions, testable theoretical propositions were formulated to connect the model’s constructs to the clinical and care dimensions of delirium.
These propositions represent an intermediate step between the theoretical and empirical levels and serve as the foundation for the subsequent development of the C-T-E structure.
A graphical representation of the structure, synthesizing the conceptual linkages and theoretical relationships identified, is presented in the results section.
3. RESULTS
The authors and other nurses have used the DSM to conceptualize symptoms and study the relationships between antecedents, experience, and nursing interventions that influence the experience and consequences of the symptoms [12]. Further, the DSM aims to improve patient outcomes by addressing the complex nature of symptoms, concomitant symptoms, their interactions, and longitudinal trajectories that change over time [11, 12]. Thus, reducing delirium using the DSM requires a holistic approach that includes active patient and family participation and interaction with the environment.
As proposed by the DSM authors, models and theories provide a logical framework for testing novel ideas, aligning statistical methods, facilitating research, and translating results into improvements in patient care [11]. Therefore, they have proposed a theoretical structure that directs the development of nursing interventions. It extends to the family’s interaction with the patient and considers demographic, physiological, psychological, social, spiritual, and environmental factors. It is an integral and holistic vision.
The theory does not specify interventions; however, it does provide guidelines for nurses to develop interventions grounded in clinical reality and aligned with the proposed theoretical structure, which, although has been used mainly in cancer patients, has theoretical constructs that can be applied to events such as Delirium.
In assessing the use of this theory, it was found to have been cited in studies employing qualitative [16, 17] and quantitative approaches, the latter involving observational designs [18-21]. It has also been applied in literature reviews and theoretical and interactive studies [13, 22, 23], while two studies were intervention-based [24, 25]. Hence, nurses should develop more studies that test theoretical and empirical concepts and contribute to the knowledge of both measurement phenomena and theory.
Based on the DSM, psychological symptoms and their impact on quality of life were studied through independent studies and in patients with oncological pathologies [18-22, 25]. In the case of Delirium, the patient experiences psychological changes such as suffering, anxiety, uncertainty, fear, and distress [26]. Thus, the approach to delirium from this theoretical perspective is beneficial for psychological recovery, which is as important as physical recovery [26].
Therefore, given that the published theory primarily comprises conceptual and theoretical elements, an analysis was conducted to understand the theory and its application to Delirium. Based on Fawcett's guidelines [1], this study developed the C-T-E, as shown in Fig. (1). Through this analysis, some conceptual (C) and theoretical (T) propositions were identified to derive the empirical aspects, and these propositions led to the elements that underpin the interventions.
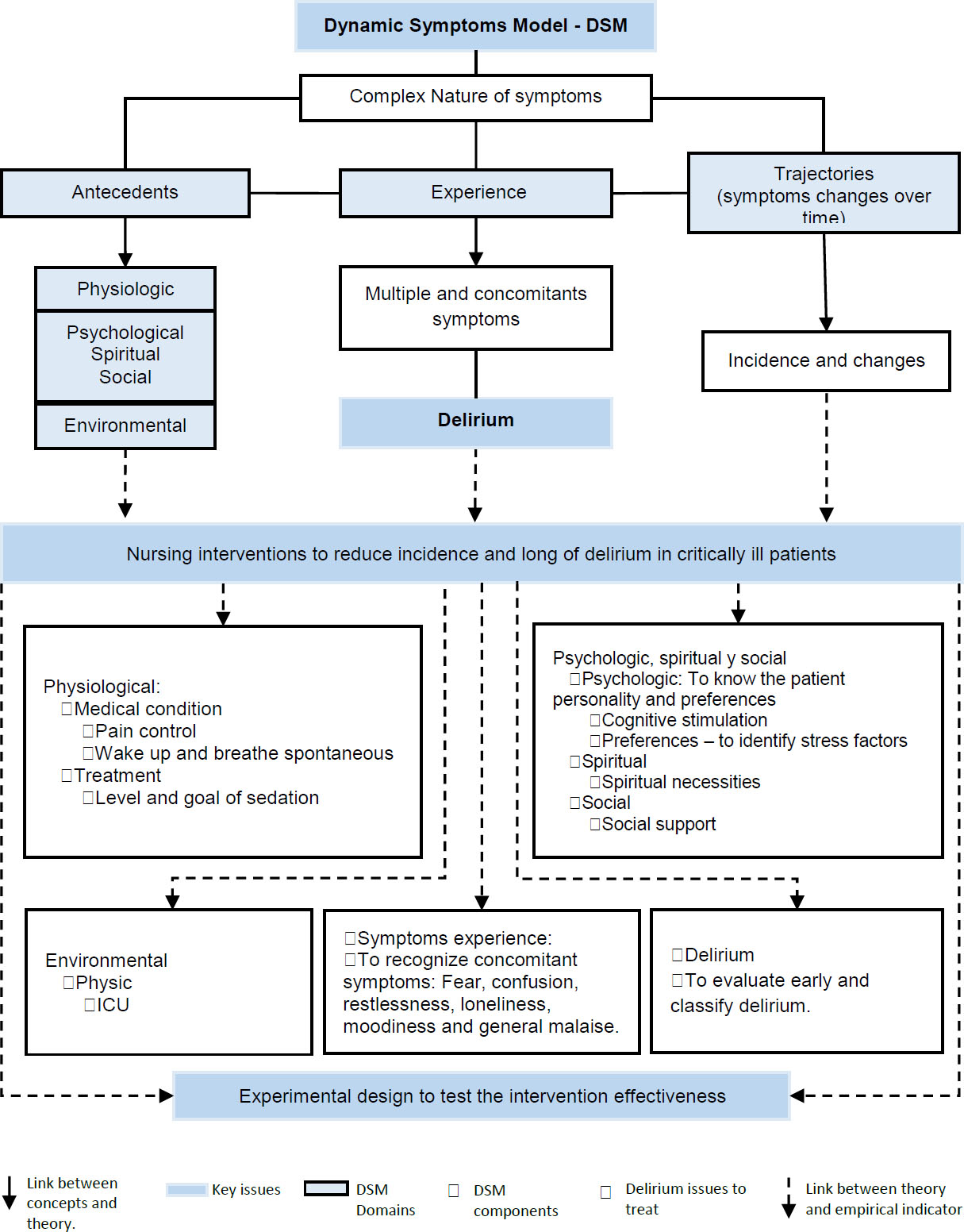
C-T-E for developing nursing interventions to reduce the incidence and duration of delirium in intensive care patients, from the DSM.
3.1. Relational Proposition for Component C of the C-T-E Structure
- Symptoms are complex and depend on the individual's history and changing trajectories [11].
Non-relational propositions for component T of the C-T-E structure are as follows:
3.2. Relational Propositions for Component E of the C-T-E Structure
3.2.1. Background
3.2.1.1. Physiological Factors
Physiological antecedents are the pathologies and treatment-related factors that promote delirium in intensive care patients, such as pain, mechanical ventilation, and medication. However, some of these can be modified to reduce their ability to trigger delirium. Adequate pain management includes regular pain assessment and timely treatment, which improve physical functioning, psychological and emotional state, and social interactions, thereby reducing the risk of delirium and promoting early awakening, respiration, and mobility [27].
Through interaction, nursing interventions can be expanded from the nurse to the care team and the patient's family [12], both in routine care [27] and in decision-making and treatment planning [28].
Mechanical ventilation is a clinical condition that potentiates delirium in intensive care patients; this impact can be minimized by awakening and spontaneous breathing, actions in which the family can participate.
Pharmacological treatment, mainly based on sedatives and analgesia with benzodiazepines, causesa medical condition that triggers delirium. This aspect can be monitored frequently through daily sedation goals, timely titration, and measurement of the degree of sedation. Thus, over- sedation can be avoided, favoring spontaneous awakening, breathing, mobility, and patient interaction.
3.2.1.2. Psychological Factors, Spiritual, and Social
Psychological antecedents are shaped by values, life experiences, and personality, which influence people in intensive care and their recovery process [12]. These factors influence people in intensive care and their recovery process. Therefore, their consideration and inclusion in patients’ self-care promote a familiar environment in the ICU and reduce stress. The social life of people in intensive care is centered on their families, who play a leading role in preventing Delirium by providing greater confidence and security to patients and reducing stress. Thus, families can be considered part of the care team, maintaining close relationships and interactions with patients.
Nursing must address the spiritual background and needs of people in intensive care as a humanization strategy. It promotes self-recognition, self-realization, and emotional balance, which can reduce delirium.
3.2.1.3. Environmental Factors
The environment influences how the person experiences the health and recovery process. This environment is largely altered in the ICU compared to that at home, which favors the development of delirium. It is necessary to adapt to it so that it is not hostile but, on the contrary, provides tranquility, rest, and comfort. The person's mobility in intensive care is altered by their health condition and the ICU environment. Therefore, the health team should encourage and initiate early mobility in patients based on their pathophysiological conditions. It helps patients feel more active, improves oxygenation, and reduces delirium risk by integrating them into their recovery.
4. DISCUSSION
The results of this work confirm the relevance of integrating nursing theory and clinical practice for the understanding and management of delirium. The development of the Conceptual-Theoretical-Empirical structure based on the Dynamic Symptoms Model demonstrated consistency between the theoretical principles of the model and the characteristics of the phenomenon, providing a comprehensive and dynamic view of delirium.
Brant and colleagues [11, 12] clarified that these indicators are dynamic and multifaceted, and that they must be viewed in light of their temporal evolution, their transformations, and the factors that drive them. Applying this perspective to delirium helps us understand that changes in a patient's thoughts and behavior arise from the interaction among predisposing factors, the nature and context of the symptoms, and the patient's environment.
This explanation is consistent with the findings of a study by Gómez et al. [13], who demonstrated a conceptual relationship between the Dynamic Symptoms Model and the clinical features of delirium, suggesting that it could be applied to build specific nursing interventions. In the same way, the theoretical propositions of this research recommend that delirium can be prevented or reduced through interventions targeting modifiable factors, such as environmental control, orientation support, and family involvement.
Our results are congruent with the current literature [8, 9], which identifies non-pharmacological interventions as an important component of delirium prevention in intensive care. Moreover, evidence reported by Mart et al. [6] corroborates that changes in environmental factors and reductions in physical and psychological stress considerably decrease the incidence of delirium.
From a theoretical viewpoint, the C-T-E structure developed here connects abstract concepts to observable variables, thus providing a logical basis for future experimental validation.
This vision aligns with Fawcett [2], who argues that the paradigm of nursing must continuously reexamine the experimental and research model and adapt it to nursing practice. This approach brings together the conceptual, theoretical, and empirical parts of the discipline, following its main principles. By combining these elements, the model becomes a useful tool for organizing and assessing nursing care. This model has proven appropriate for a comprehensive care strategy because it combines physical, psychological, interpersonal, and environmental factors.
The theory and the theoretical propositions developed by linking the DSM to delirium were tested in a controlled clinical trial. The interventions were compared between an intervention group that received care based on the DSM and scientific evidence and a control group that received routine care. This study demonstrated better outcomes in the intervention group, with a lower incidence and duration of delirium, lower pain intensity, less time spent in physical restraints, fewer days on mechanical ventilation, and a shorter length of stay in the ICU [29].
The DSM was also applied to address delirium in the pediatric population. The results of the present study show similarities with findings in the pediatric population, as the DSM enabled understanding and analysis of delirium from a holistic perspective, considering the physical, psychological, spiritual, social, occupational, and family factors underlying it [30].
Esquivel-Garzón et al. [31] concur, emphasizing that the health sciences can demonstrate the complexity of clinical practice and guide its application through appropriate and flexible models. Another advantage of the proposed system is that it provides a common working language. Although the NNN taxonomy (NANDA-I, NIC, NOC) is not the main objective of the research, a theory-driven conceptual framework can be a useful tool for guiding its application in clinical observations, interventions, and outcomes [14, 15].
The results presented here provide nursing schools with evidence supporting the teaching of epistemological and theoretical nursing knowledge in clinical practice. Therefore, they can serve as a reference for learning and applying this framework, as well as for analysis when addressing delirium as a phenomenon in clinical practice, academia, and research. Thus, the next step in the research context from this theoretical perspective is to continue developing and testing the theoretical propositions and to enrich the NNN taxonomy regarding delirium, thereby facilitating its application in academia and clinical practice.
The practice implications of this study allow us to understand delirium as an event in which the patient's various antecedents converge, creating a particular experience. Furthermore, this finding also applies to the different types of delirium, such as hypoactive, hyperactive, and mixed, since they have similar neurobiological mechanisms and share some etiological factors, whether modifiable or non-modifiable [31]. Therefore, nurses can apply DSM to reduce delirium in patients and address delirium antecedents, tailoring interventions according to the antecedents identified.
Finally, this approach is consistent with the recommendations of Fawcett & DeSanto-Madeya [1], who state that the consistent application of theoretical models in practice strengthens the interpretation of practice and establishes evidence-based, theory-guided nursing [1].
A background based on ideas, knowledge, and research provides the foundation for establishing health measures to prevent disease. This provides a framework for translating theories into practice, teaching, research, and clinical practice. According to Fawcett [1], nursing theory provides a framework to guide clinical judgment and ensure quality care. Using an evidence-based approach, nurses can significantly contribute to preventing cognitive impairment, safeguarding patients' cognitive and functional abilities, and ensuring the overall quality of care.
5. STUDY LIMITATIONS
More research is needed to apply and test the nursing theoretical propositions regarding delirium phenomena or other topics relevant to nursing care.
CONCLUSION
The theoretical and empirical foundations described in this paper contribute to the theory of patient care by introducing a dynamic symptoms model of delirium and translating theoretical concepts into recommendations for patient care, by aligning the main concepts of the model in this work with the care needs of patients with compromised consciousness. The theoretical framework offers suggestions for expanding inclusive, person-centered healthcare and reducing the gap between theory, research, and nursing practice, thereby enhancing understanding of the phenomenon. The indirect research methodology used goes beyond a purely empirical approach and contributes to evidence-based practice.
The conceptual-theoretical-empirical (C-T-E) structure provides a logical, sequential framework for applying theory in practice, enabling the development of interventions grounded in disciplinary knowledge and consistent with the theoretical elements of the phenomena. It provides a holistic perspective on the human being. Consequently, its application benefits patients, their families, and the discipline of nursing. In critically ill patients' care, this approach supports nursing care by integrating physical, psychological, social, and environmental factors. More empirical research is required to test the relationship between theoretical concepts and to assess the effectiveness of care built from the proposed model. Then, this framework provides a foundation for nursing practice and contributes to professional growth and the improvement of care quality by integrating nursing theory, research, and practice.
AUTHORS’ CONTRIBUTIONS
The study was initially designed by A.M.H.C. and L.O.G.T., and subsequently discussed with C.I.A.G., M.G.C., M.T., and G.G. The methodology was defined by A.M.H.C., C.I.A.G., and L.O.G.T. A.M.H.C. and L.O.G.T. conducted the analysis. The results were discussed collectively by all authors. C.I.A.G., M.G.C., M.T., and G.G. drafted the manuscript, while A.M.H.C., C.I.A.G., and L.O.G.T. critically revised it. All authors read and approved the final manuscript.
LIST OF ABBREVIATIONS
| C-T-E | = The conceptual-theoretical-empirical |
| ICU | = Intensive Care Unit |
| DSM | = Dynamic Symptoms Model |
| NNN | = NANDA-I, NIC, NOC |
AVAILABILITY OF DATA AND MATERIALS
All the data and supporting material are available within the article.
CONFLICT OF INTEREST
The authors declare no financial or personal conflicts of interest that could have influenced the work presented.
ACKNOWLEDGEMENTS
The authors acknowledged the universities and colleagues who led the development of this job.