All published articles of this journal are available on ScienceDirect.

The Effect of SITERDUGA on Family Anxiety: A Quasi-Experimental Study
Authors Info & Affiliations
Abstract
Background
Family Caregivers (FCG) play a crucial role in the recovery process of individuals with Severe Mental Disorders (SMDs). The negative stigma against people with SMDs and their families leads to their isolation, which results in insufficient support from the family in the recovery process. FCGs who care for members with SMD are at risk of experiencing anxiety. This condition requires proper management. Moreover, the use of Android-based applications is growing in parallel with the increasing use of smartphones in daily life, and these applications can address psychological issues.
Objective
The purpose of this study was to analyze the effect of the SITERDUGA application on the anxiety levels of FCGs caring for people with SMD.
Methods
This study employed a quasi-experimental design with pre-test and post-test control groups. The study was conducted from September to November 2024 in Denpasar City, Indonesia. The population of people with SMDs was 231 people. The sampling technique was purposive sampling, with a sample of 80 people divided into two groups of 40 participants each. The participants were assigned to each group randomly. The study measured anxiety levels using the STAI-T questionnaire. The intervention group then received training using the application SITERDUGA (Integrated Information System for the Movement to Support and Accept People with Mental Disorders in the Family). The application consists of RISA (Mental Health Information Room), NOTA (Care Notification), AKTA (Family Modality Activity), and DETIK (Family Integrated Emotional Support).
Results
The results of this study showed a change in anxiety levels among respondents before and after the intervention using the SITERDUGA application. In the intervention group, the p-value was 0.000, while the control group had a p-value of 0.051, meaning no change occurred without treatment. The intervention provided through the comprehensive approach, such as the SITERDUGA application, was able to reduce the anxiety experienced.
Conclusion
The SITERDUGA application could be a useful guide to support families in taking care of patients with SMD.
1. INTRODUCTION
Many Indonesians are still unaware of the importance of mental health [1]. Schizophrenia is a common mental disorder that affects individuals physically, emotionally, and socially [2]. According to WHO, over 450 million people globally suffer from mental disorders, with schizophrenia accounting for 13% of all cases, a figure projected to rise to 25% by 2030 [3, 4]. In Indonesia, 282,654 households, or 0.67% of the population, experience schizophrenia, with the prevalence in Bali rising from 2.3 to 11.1 per thousand between 2013 and 2018 [3].
Family involvement plays a critical role in supporting schizophrenia patients by providing care, motivation, and monitoring. However, caregiving often burdens families, leading to stress, depression, and anxiety [5, 6]. Families of individuals with Severe Mental Disorders (SMDs) face high levels of anxiety due to societal stigma, lack of understanding, and the long-term nature of care [7, 8]. High anxiety can negatively affect both the caregiver and the patient, leading to inadequate care, conflict, and even harmful practices like seclusion or confinement [9, 10].
Interventions have been developed to support families, and this study introduces SITERDUGA, an innovative information system designed to reduce family anxiety by offering resources, psychosocial support, and practical guidance for managing SMD. A preliminary study at Denpasar Utara III Health Center, which has a high prevalence of mental disorder cases, revealed significant family anxiety. SITERDUGA aims to address this by improving the mental health of the family and enhancing patient care. Therefore, the purpose of this study was to analyze the effect of the SITERDUGA application on the level of anxiety in families with SMD.
2. METHODS
2.1. Study Design
This study employed a quasi-experimental design with a pre-test and post-test control group structure using a quantitative approach [11]. The research aimed to compare the effects of the SITERDUGA application on the anxiety levels of families caring for individuals with Mental Disorders (SMD) against a control group receiving standard education based on the Health Center's Standard Operating Procedures (SOP). The study was conducted at the Denpasar Utara III Health Center, Bali, from June 2024. It was structured in two phases: the pre-test phase, which involved collecting baseline data on family anxiety levels, and the post-test phase, which evaluated the effects of the intervention.
2.2. Study Population and Sampling
The study population consisted of 231 individuals diagnosed with SMD registered at the Denpasar Utara III Health Center. Purposive sampling was used to select the study participants. Families who met the inclusion criteria were those who cared for individuals with SMD, experienced anxiety, and were willing to participate in the study by signing an informed consent form. They also had to be able to read and write, own an Android-based mobile phone, and be willing to undergo training on using the SITERDUGA application. The exclusion criteria included families who were unable to attend the pre-test or post-test or those who could not complete the training sessions on the application.
The study used G*Power to calculate the sample size. The mean difference between the two independent means was set with an effect size of 0.8, α = 0.05, power = 0.95, and an allocation ratio (N2/N1) of 1. The results showed that the minimum sample size of each group was 35. The ten percent attrition rate was considered to avoid a loss to follow up below the minimum sample size. The total sample size was 80 participants divided equally in each group.
A total of 80 families who met the inclusion criteria were randomly assigned to either the treatment group, which consisted of 40 families who received the SITERDUGA application intervention, or the control group, also comprising 40 families, who received the standard education provided by the Health Center.
2.3. Data Collection and Intervention
The study was conducted over three months, starting in June 2024. The design, testing, and validation of the SITERDUGA application were completed before the start of the intervention. Data collection occurred during the final month, with the total intervention period spanning 14 days for each participant group.
The SITERDUGA application was developed based on these principles by providing interactive educational materials, discussion forums, and reminders of care tasks that can improve FCG self-efficacy and well-being. The SITERDUGA application was tested on 10 Family Caregivers (FCGs). They could use and accept any features of the application correctly.
Before technology-based interventions were introduced, educational sessions for FCGs were typically con>ducted through seminars, lectures, or printed guidebooks, but these methods have several limitations. Lack of accessibility can be a major issue, as FCGs may not always be able to attend face-to-face educational sessions due to time and location constraints. Additionally, these traditional methods often lack interactivity, making the materials less engaging and unable to provide immediate feedback. Another significant drawback is the limited ongoing support, as caregivers may struggle to remember information or seek help once the educational sessions are completed.
The treatment group participated in an intervention using the SITERDUGA application, which was developed as a comprehensive tool to assist families in managing the care of SMD patients at home. The families in the treatment group were provided with training on how to use the SITERDUGA application. This application included four key features designed to aid families in managing their anxiety and providing care:
1. RISA (Mental Health Information Room), which provided educational videos on mental health aimed at helping families understand the fundamentals of SMD care.
2. NOTA (Care Notification), a reminder system that helped families organize care by notifying them about medication schedules, appointments, and key contacts at the Health Center.
3. AKTA (Family Modality Activity), which included a guided therapy module for performing Emotional Freedom Technique (EFT) to reduce anxiety. Families were instructed to complete 15-minute EFT sessions daily for two weeks.
4. DETIK (Integrated Family Emotional Support), which facilitated mutual support among families, allowing them to share inspirational stories and recommendations to combat the stigma associated with mental disorders.
According to its SOP for mental health care, the control group received standard education materials and sessions provided by the Public Health Center. The intervention period lasted for two weeks, during which the families in the treatment group used the SITERDUGA application six times. After two weeks, both groups were reassessed to evaluate changes in anxiety levels.
Data were collected using structured questionnaires administered at two-time points: before the intervention (pre-test) and after the intervention (post-test). The instruments included a demographic questionnaire, a sociodemographic survey, and the State-Trait Anxiety Inventory-Trait (STAI-T) questionnaire. The STAI-T questionnaire was chosen because it is a validated tool for measuring anxiety levels and is easy to understand by families caring for individuals with mental disorders. The STAI-T consists of 20 items with scores ranging from 20 to 80, which were categorized as normal (20–29), mild anxiety (30–39), moderate anxiety (40–49), and severe anxiety (50–80). The STAI-T instrument had been previously tested for validity (interval value of 0.88) and reliability (Cronbach’s alpha of 0.86).
Eighty patients in intervention and control groups were analyzed. There was no lost to follow up on each group. The details of patient flow can be seen in Fig. (1).
2.4. Data Analysis
The collected data were analyzed using statistical tests to determine the impact of the intervention. First, the normality of the data was tested using the Kolmogorov-Smirnov test. The homogeneity of variance was tested using Levene’s test. Parametric tests were applied, including paired t-tests to compare pre- and post-intervention anxiety levels within each group and independent t-tests to compare the differences between the treatment and control groups. Multivariate analyses of the covariate test (Manova) were performed to ensure whether the demographic variables had an effect on the intervention. Cohen's d was calculated to determine the effect size between the two groups. Cohen classified effect sizes as small (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8) [12].
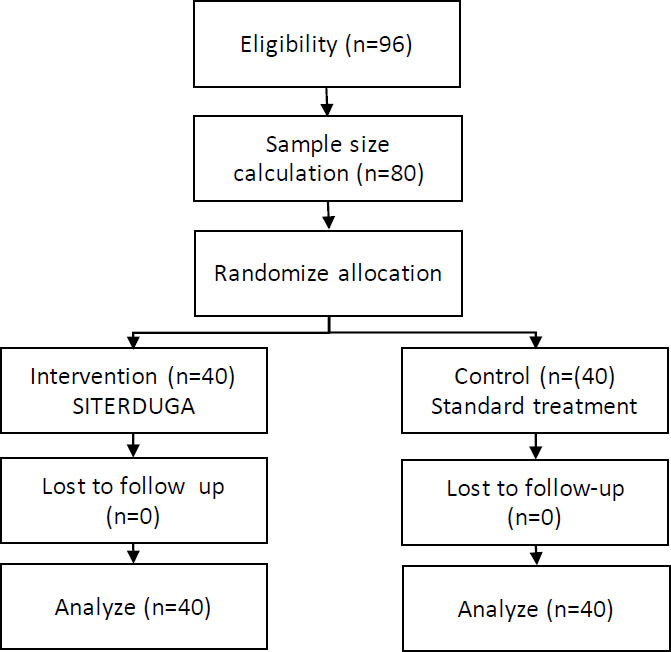
Flow of patients through the study for SITERDUGA.
2.5. Ethical Considerations
This study was approved by the Health Research Ethics Committee of the National Research and Innovation Agency (Approval No: 178/KE.03/SK/09/2024) and issued on September 17, 2024. Prior to participation, all respondents were given a clear explanation of the study's objectives, benefits, procedures, and confidentiality measures. Informed consent was obtained from each participant. Participation was voluntary, and those who chose not to participate were not pressured. The confidentiality of all data provided by the respondents was ensured, and the information was used solely for research purposes.
3. RESULT
3.1. Respondent Characteristics
The study examined participants in control and intervention groups, focusing on gender, age, education, occupation, and caregiving experience (Table 1). Most participants were women (62.5% control, 65% intervention), and both groups had a similar age distribution, with the majority in early adulthood. High school graduates predominated (60% control, 62.5% intervention), and most worked in the private sector. None had prior caregiving experience, and all were from urban areas.
Anxiety levels were comparable before the intervention, with moderate to severe anxiety common in both groups. After the intervention, anxiety worsened in the control group, while the intervention group showed significant improvement. The Levene’s Test indicated unequal variances, but the t-test showed a statistically significant difference (p=0.000) in post-intervention anxiety (See Table 2). The intervention group had anxiety scores that were 9.45 points lower than the control group, with a high effect size (d = 4.51), indicating a strong impact of the intervention. Demographic factors did not significantly influence anxiety reduction, which was primarily attributed to the intervention.
| Respondent Characteristics | Control Group | Intervention Group | ||
|---|---|---|---|---|
| Frequency (f) | Percentage (%) | Frequency (f) | Percentage (%) | |
| Gender | - | - | - | - |
| Male | 15 | 37.5 | 14 | 35.0 |
| Female | 25 | 62.5 | 26 | 65.0 |
| Age | - | - | - | - |
| Early adult (26-35 years) | 13 | 32.5 | 15 | 37.5 |
| Late adult (36-45 years) | 12 | 30.0 | 11 | 27.5 |
| Early Older Adult (46-55 years) | 11 | 27.5 | 12 | 30.0 |
| Late Older Adult (56-55 years) | 4 | 10.0 | 2 | 5.0 |
| Education | - | - | - | - |
| Junior High School Graduate | 13 | 32.5 | 12 | 30.0 |
| High School Graduate | 24 | 60.0 | 25 | 62.5 |
| College | 3 | 7.5 | 3 | 7.5 |
| Occupation | - | - | - | - |
| Civil servant | 2 | 5.0 | 4 | 10.0 |
| Private | 24 | 60.0 | 22 | 55.0 |
| Self-employed | 14 | 35.0 | 14 | 35.0 |
| Experience in caring for SMDs | - | - | - | - |
| Yes | 0 | 0 | 0 | 0 |
| No | 40 | 100 | 40 | 100 |
| Demographic environment | - | - | - | - |
| Urban | 40 | 100 | 40 | 100 |
| Rural | 0 | 0 | 0 | 0 |
| Pretest | - | - | - | - |
| Mild Anxiety | 2 | 5.0 | 2 | 5.0 |
| Moderate Anxiety | 18 | 45.0 | 17 | 42.5 |
| Severe Anxiety | 20 | 50.0 | 21 | 52.5 |
| Posttest | - | - | - | - |
| Normal | 0 | 0 | 1 | 2.5 |
| Mild Anxiety | 1 | 2.5 | 12 | 30.0 |
| Moderate Anxiety | 17 | 42.5 | 20 | 50.0 |
| Severe Anxiety | 22 | 55.0 | 7 | 17.5 |
| Variable | Group | p-value | p-value |
|---|---|---|---|
| Paired T-Test | Independent T-Test | ||
| Anxiety | Control | 0,051 | <0,001 |
| Intervention | <0,001 |
The MANOVA test results showed that the intercept was greater than 0.05 (shown in Table 3), indicating that demographic factors, such as age, gender, education, occupation, and caregiving experience, did not significantly influence the effectiveness of the intervention.
4. DISCUSSION
The results of this study highlight the significant impact of the SITERDUGA application-based intervention in reducing anxiety levels among families caring for individuals with Severe Mental Disorders (SMD). The intervention group showed a statistically significant decrease in anxiety compared to the control group, as indicated by the independent samples t-test results (t = -5.716, p = <0.001). Additionally, the effect size of 4.51 suggests a high effect, demonstrating the application's effectiveness in alleviating anxiety symptoms.
The reduction in anxiety observed in the intervention group aligns with previous studies showing that structured psychosocial interventions can effectively alleviate caregiver anxiety. The application provided practical support, such as reminders for patient care, educational resources on mental health, and emotional support, all of which are critical components of caregiving. According to Chien and Norman (2009), family interventions that offer psychoeducation and emotional support can significantly reduce
| Parameter | B | Std. Error | t | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Intercept | 3.500 | 1.788 | 1.957 | 0.064 | -.231 | 7.231 |
| Age | - | - | - | - | - | - |
| Early adult (26-35 years) | 5.600 | 2.023 | 2.768 | 0.012 | 1.379 | 9.821 |
| Late adult (36-45 years) | 7.167 | 3.362 | 2.132 | 0.046 | 0.154 | 14.179 |
| Early Older Adult (46-55 years) | 4.500 | 2.116 | 2.127 | 0.046 | 0.086 | 8.914 |
| Late Older Adult (56-55 years) | Parameter | |||||
| Gender | - | |||||
| Male | -1.500 | 1.385 | -1.083 | 0.292 | -4.390 | 1.390 |
| Female | Parameter | |||||
| Education | - | |||||
| Junior High School Graduate | 2.500 | 2.116 | 1.181 | 0.251 | -1.914 | 6.914 |
| High School Graduate | 1.000 | 1.600 | 0.625 | 0.539 | -2.337 | 4.337 |
| College | Parameter | |||||
| Occupation | - | |||||
| Civil servant | 3.000 | 1.600 | 1.875 | 0.075 | -0.337 | 6.337 |
| Private | 0.500 | 1.131 | 0.442 | 0.663 | -1.859 | 2.859 |
| Self-employed | Parameter | |||||
| Experience in caring for SMDs | - | |||||
| Yes | -4.500 | 2.116 | -2.127 | 0.046 | -8.914 | -0.086 |
| No | Parameter | |||||
caregiver burden and anxiety [13, 14]. The SITERDUGA application addressed these needs through its integrated features, such as RISA (Mental Health Information Room), NOTA (Care Notification), AKTA (Family Modality Activity), and DETIK (Family Integrated Emotional Support). These resources equipped families with knowledge and tools to manage both patient care and their own psychological well-being, which could explain the significant reduction in anxiety.
One of the key strengths of the intervention was its accessibility and the ability to deliver psychoeducation and emotional support through a mobile platform. This feature aligns with the growing body of literature on the effectiveness of mobile health (mHealth) interventions in supporting caregivers. Studies have shown that mHealth applications can provide real-time support, reduce stress, and enhance the quality of life for caregivers of individuals with chronic conditions [15, 16]. The ability of caregivers to access the application at their convenience may have helped reduce the burden associated with caregiving, contributing to the reduction in anxiety levels.
Interestingly, the MANOVA test results indicated that demographic factors, such as age, gender, education, occupation, and caregiving experience, did not significantly influence the effectiveness of the intervention (p > 0.05). This suggests that the SITERDUGA intervention was equally effective across different demographic groups, demonstrating its broad applicability. This finding contrasts with previous studies where caregiver characteristics, such as age and gender, were found to impact caregiver burden and mental health outcomes [17, 18]. The lack of significant influence from demographic variables in this study could be attributed to the comprehensive nature of the application, which provided tailored support that transcended these individual differences.
The consistency of the effectiveness of the intervention across different demographic groups is important for its scalability and potential for widespread implementation. As mental health caregiving is a role often filled by individuals from diverse backgrounds, the ability of a single intervention to meet the needs of various groups without modification makes it a valuable tool for broader public health strategies aimed at reducing caregiver burden.
In comparison to the control group, which received standard care in line with health center protocols, the intervention group experienced a notable decrease in severe anxiety (from 52.5% pretest to 17.5% post-test). This finding reinforces the limitations of standard care in addressing the psychological needs of families caring for SMD patients. Standard care often focuses on the clinical management of the patient’s condition and may not adequately address the emotional and psychological burden experienced by caregivers [19, 20]. The SITERDUGA application, by contrast, provided comprehensive support that went beyond patient care, focusing on the caregiver's mental health and offering tools for stress and anxiety management, which is likely the key factor behind its success.
5. IMPLICATIONS FOR PRACTICE AND POLICY
The significant reduction in anxiety among caregivers in the intervention group has important implications for mental health policy and caregiving practices. Caregivers play a critical role in the management of mental health conditions, and high levels of anxiety can negatively affect their ability to provide effective care, as well as their own well-being. By reducing caregiver anxiety, interventions like SITERDUGA can improve not only the quality of life for caregivers but also patient outcomes. This aligns with the findings of Perlick et al. (2001), which suggest that reducing caregiver distress can lead to better patient adherence to treatment and fewer relapses in individuals with mental disorders [21].
Given the high effect size observed in this study, integrating the SITERDUGA application into routine mental health care for SMD patients could be a cost-effective and scalable solution to address the emotional needs of caregivers. Policymakers and healthcare providers should consider adopting similar mHealth interventions as part of a comprehensive mental health strategy. This is particularly important in low- and middle-income countries like Indonesia, where access to mental health services is often limited, and caregivers bear a significant portion of the care burden.
6. LIMITATIONS
While the study demonstrated the effectiveness of the SITERDUGA application, several limitations exist. First, the study was conducted over a relatively short period (two weeks), and it is unclear whether the observed reduction in anxiety would be sustained over a longer duration. Long-term follow-up studies are needed to assess the persistence of these effects. Second, the generalizability of the findings is also limited due to the study population being restricted to a specific demographic group with access to digital resources. Future research should explore whether similar interventions would be effective in different settings and among caregivers with different technology access levels.
Additionally, while the intervention reduced anxiety, the study did not measure other aspects of caregivers’ well-being, such as depression or physical health. Therefore, future studies should explore the broader impact of mHealth interventions on various dimensions of caregiver health and well-being.
CONCLUSION
The effectiveness of the SITERDUGA application can be attributed to its comprehensive features, including psychoeducation, care reminders, and emotional support, which collectively empowered caregivers in managing both patient care and their own psychological well-being. The accessibility of the intervention through a mobile platform facilitated convenience, reinforcing the growing evidence supporting mHealth solutions as viable tools for mental health support.
Furthermore, a notable finding of this study is the lack of significant influence of demographic factors on intervention effectiveness. Regardless of age, gender, education level, occupation, or caregiving experience, all participants benefited from the intervention. This highlights the broad applicability and scalability of the SITERDUGA application, making it a promising tool for diverse caregiver populations.
AUTHORS’ CONTRIBUTIONS
N.M.N.W.: Contributed to the conception and design of the study; N.M.N.W., P.I.D., N.L.P.T.D., A.A.S.S., N.L.P.D.P., and I.N.D.W.: Contributed to data acquisition and data analysis; N.M.N.W. and Y.A.: Wrote the first draft of the manuscript and revised the final draft. All authors approved the final version of the article to be published and agreed to be accountable for each step of the study.
LIST OF ABBREVIATIONS
| FCG | = Family Caregivers |
| SMDs | = Severe Mental Disorders |
| SOP | = Standard Operating Procedures |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study approval was obtained from the Health Research Ethics Committee, National Research and Innovation Agency (Approval number: No: 178/KE.03/SK/09/2024 on 17 September 2024).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article. The datasheet is attached in the supplementary file.
FUNDING
This study was funded by the Ministry of Education, Culture and Technology of Indonesia, grant number 0459/E5/P6.02.00/2024.
ACKNOWLEDGEMENTS
The authors would like to thank the participants in this study and Puskesmas III Denpasar Utara for their partnership in this research.