All published articles of this journal are available on ScienceDirect.

Intervention to Enhance Resilience among Nurse Managers: A Systematic Review
Authors Info & Affiliations
Abstract
Background
Nurse managers are vital in healthcare, bridging frontline staff and administration. Their responsibilities, often associated with high stress, were intensified during the COVID-19 pandemic, highlighting the need for resilience to sustain their well-being and team management.
Aim
This systematic review assessed the effectiveness of resilience-enhancing interventions for nurse managers.
Methods
Using the keywords Leadership, Manager, and Resilience, there were seven studies involving 318 participants across the United States, Turkey, Egypt, and Brazil. Interventions included mindfulness training, psychoeducational programs, and authentic leadership development, applied through randomized controlled trials and quasi-experimental designs.
Results
The results showed that resilience-focused interventions significantly improved nurse managers' emotional intelligence, leadership skills, and psychological well-being. Programs targeting emotional intelligence components, such as self-awareness, empathy, and self-control, fostered resilience and professional efficacy. Specifically, mindfulness-based interventions enhanced emotional regulation and dispositional mindfulness, while psychoeducational and leadership programs promoted mental health and job satisfaction. The findings underscore the importance of integrating resilience-building programs into nurse manager training. Such interventions can enhance nurse managers' ability to handle stress, support their teams, and positively impact patient care outcomes. Implementing structured resilience programs may benefit healthcare organizations in terms of improved team dynamics and quality of care.
Conclusion
Resilience-building interventions are a valuable addition to nurse manager training, supporting their well-being and leadership capacity. Future research should examine the long-term effects of these programs on resilience and workforce retention.
1. INTRODUCTION
The global health crisis of 2020–2021 placed extraordinary strain on healthcare systems, with nurses at the forefront, facing immense physical, emotional, and psychological challenges. Prolonged exposure to high-stress environments, managing critically ill patients, dealing with shortages of personal protective equipment (PPE), and witnessing high mortality rates significantly impacted their well-being [1, 2]. Despite these challenges, many nurses demonstrated remarkable resilience, enabling them to provide critical care under extreme conditions. Resilience—the capacity to adapt, recover, and thrive in adversity—was vital for sustaining their well-being and maintaining continuity in healthcare services during this period [3, 4].
While much attention has been given to frontline nurses' resilience during the pandemic, the focus on nurse managers is equally important yet less explored. As leaders of the largest workforce in healthcare, nurse managers bridge the gap between administrative leadership and frontline staff. Their responsibilities include supervising teams, ensuring high standards of patient care, managing budgets, implementing policies, and addressing conflicts. These roles were amplified during the pandemic as nurse managers had to support their teams' well-being, maintain care standards, and navigate the crisis's unprecedented challenges [4, 5].
Nurse managers face unique stressors that combine leadership demands with direct and indirect exposure to workplace stress, burnout, and compassion fatigue [6]. Their performance directly impacts staff morale, team efficiency, and patient outcomes. However, existing organizational frameworks often fail to support these leaders sufficiently, leaving a gap in addressing their resilience and well-being. This gap has far-reaching implications, as nurse managers' resilience supports their well-being, enhances team dynamics, improves patient care quality, and promotes organizational efficiency.
Existing literature highlights interventions such as mindfulness training, psychoeducational programs, and leadership development initiatives as potential strategies to build resilience [5, 7, 8]. However, these interventions have not been systematically integrated into healthcare management practices, and the evidence base remains fragmented. Previous studies often focus on individual resilience traits rather than organizational strategies, limiting their applicability to real-world settings. Moreover, most research has centered on frontline nurses, with insufficient attention paid to nurse managers, whose dual roles during crises amplify their need for resilience support.
1.1. Purpose of Systematic Review
This systematic review aims to address this gap by evaluating the effectiveness of resilience-building interventions tailored explicitly to nurse managers. By analyzing evidence from randomized controlled trials (RCTs) and quasi-experimental studies, this review seeks to provide a comprehensive understanding of how interventions such as mindfulness programs, psychoeducational initiatives, and leadership development frameworks can enhance resilience. The findings will inform healthcare organizations on how to equip nurse managers better to lead effectively, especially in high-pressure environments, ultimately improving outcomes for staff, patients, and the healthcare system.
2. MATERIALS AND METHODS
This systematic review was done following the guidelines as per the PRISMA checklist [9]. Multiple databases were used, and during the preliminary search, 4,362 studies were found, with two additional studies identified through manual searches.After removing duplicates and applying inclusion criteria, 63 reports were sought for eligibility, and at the end, seven studies that were full text were included for review in this study.
2.1. Search Strategy
The review focused on studies published in English, with the search extending until June 2024. Databases such as PubMed, Ovid-MEDLINE, COCHRANE Library, ScienceDirect, and Google Scholar were searched using a comprehensive set of keywords. The searches included terms such as “resilience,” “leadership,” “management,” “nurse,” “manager,” “technique,” “approach,” “interventions,” “program,” “blind,” “trial,” “quasi-experimental,” and “RCT,” combined in various ways to capture relevant studies [10].
Grey literature and unpublished studies were explicitly excluded to maintain methodological rigor and ensure that included studies met established publication standards.
2.2. Study Eligibility Criteria
Studies included in this review should meet the following criteria:
1. The population targeted were nurse managers or nurse administrators holding leadership roles within healthcare organizations. They were responsible for managing services, supervising staff, and ensuring the delivery of nursing care to patients. Given their high-stress environments and significant responsibilities, the selected studies emphasized the importance of resilience as a critical skill for effective functioning in these roles.
2. The interventions reviewed were programs, training, or strategies explicitly designed to enhance resilience and core competencies in nurse managers. Examples of such interventions included leadership development programs, stress management workshops, and resilience-building exercises. These initiatives were tailored to address nurse manager roles' unique challenges and demands, aiming to improve their capacity to lead effectively and cope with organizational pressures.
3. The review included only studies utilizing randomized controlled trials (RCTs) or quasi-experimental designs. RCTs compared intervention groups with control groups to determine the intervention's effectiveness, while quasi-experimental studies measured outcomes within the same group before and after the intervention. This criterion ensured that the included studies provided reliable evidence regarding the interventions' impact.
4. The primary outcome of interest was the improvement of resilience in nurse managers. Secondary outcomes, such as enhanced leadership performance, improved psychological well-being, and better team dynamics, were also considered where applicable. These outcomes aligned with the review's objective to explore the role of resilience in supporting nurse managers' well-being and leadership capacity.
2.3. Study Selection
EndNote X9 software was used to manage references and remove duplicates. Two independent reviewers (HM and YPS) screened the titles and abstracts for potential inclusion, applying predefined eligibility criteria. Full-text screening was then conducted to confirm eligibility. Disagreements were resolved through discussion and, when necessary, consultation with a third reviewer (CYL), who assisted as an adjudicator. Inter-rater reliability was quantified using Cohen’s Kappa, yielding a substantial agreement (κ = 0.78).
2.4. Data Extraction
In accordance with the Cochrane guideline, the data extraction procedure started with a standardized form created to record the following crucial study information: author, year, participant demographics, intervention details, control conditions, outcome measures, and study design. Two separate authors (HM and YPS) carried out the essential extraction procedure. Following independent data extraction, one author (HM) noted potential biases and recorded summary statistics (e.g., means, SDs, effect sizes), while the second author (YPS) verified the accuracy, resolving discrepancies through a third-party consultation.
2.5. Risk of Bias Assessment
The risk of bias in RCTs was evaluated using the Cochrane Collaboration Risk of Bias tool [11]. The assessment covered the following domains: random sequence generation, allocation concealment, blinding of participants, personnel, and outcome assessors, incomplete outcome data, selective reporting, and other sources of bias.
All RCTs included in the review were rated as low risk for random sequence generation, as randomization was conducted using computer-generated methods or simple draws. However, due to the nature of the interventions, none of the studies fully blinded participants and personnel, introducing moderate performance bias. Outcome assessments were primarily self-reported, which further contributed to potential detection bias.
The ROBINS-I (Risk of Bias in Non-Randomized Studies of Interventions) tool was applied for quasi-experimental studies [12]. The evaluated domains included confounding, participant selection, classification of interventions, deviations from intended interventions, missing data, outcome measurement, and reported results selection.
Most quasi-experimental studies demonstrated a moderate risk of bias, primarily due to confounding variables and incomplete outcome data.
3. RESULTS
3.1. Characteristics of Included Studies
A comprehensive database search identified 4,362 studies, with two additional from manual searches. After removing duplicates and applying inclusion criteria, seven studies involving 318 nurse managers (223 intervention; 95 control) met the eligibility requirements. These studies were conducted in the United States (n=4), Turkey (n=1), Egypt (n=1), and Brazil (n=1) (Fig. 1). While the geographical diversity highlights resilience-building interventions across different healthcare contexts, the concentration of studies in the U.S. limits generalizability, particularly in low-resource settings.
3.2. Study Sample Sizes
The total sample size across the reviewed studies was 318 participants, with individual cohorts ranging from 20 to 85 participants. This relatively small sample size limits statistical power and the ability to detect subtle but meaningful effects of interventions. The risk of bias was evaluated using the Cochrane Risk of Bias tool for RCTs and the ROBINS-I tool for quasi-experimental studies [11, 12]. While RCTs exhibited low risk for randomization methods, they faced moderate risks related to blinding, given the nature of the interventions. Performance and detection biases were evident, particularly in studies relying on self-reported outcomes. Quasi-experimental studies were rated as a moderate risk due to confounding variables, challenges in classifying interventions, and instances of missing data. Overall, the small sample sizes and dependence on self-reported outcomes heightened the potential for reporting bias, reducing the robustness and generalizability of findings.
3.3. Interventions and Effectiveness
A range of interventions targeting resilience, leadership skills, and mental well-being among nurse managers was explored, with varying levels of methodological quality and effectiveness. The Web-Based Crisis Management Training Program by Alan et al. 2023, focused on crisis management, stress reduction, and team motivation, yielding significant post-intervention knowledge improvements (t = 4.982, p < 0.001), though its generalizability was limited by being conducted during the COVID-19 pandemic [13].
Mindfulness-based interventions by Santos et al. [14] improved emotional intelligence and resilience, showing significant gains in sociability (p=0.009), self-control (p=0.015), and mindfulness (p=0.026), with moderate to large effect sizes. Authentic Connections Group by Chesak et al. [15] emphasized work-life balance, stress reduction, and self-compassion, achieving significant effects for depression reduction (η2p = .20) and moderate effects for personal accomplishment (η2p = .13). However, emotional exhaustion improvements were minor (η2p = .03). The strength-based coaching program by Spiva et al. [16] enhanced transformational leadership and resilience significantly (F = 39.40, p < .001 and F = 22.32, p < .001, respectively) but lacked follow-up data.
Psychoeducational group programs reduced stress and burnout while increasing empowerment (t=-2.86, p=0.007) but did not significantly affect resilience scores (F=0.015, p=0.93) [16]. Lastly, the Authentic Leadership and Mindfulness Program showed substantial improvements in leadership and mindfulness (p=0.001), with large effect sizes [18]. Despite moderate to large effect sizes reported
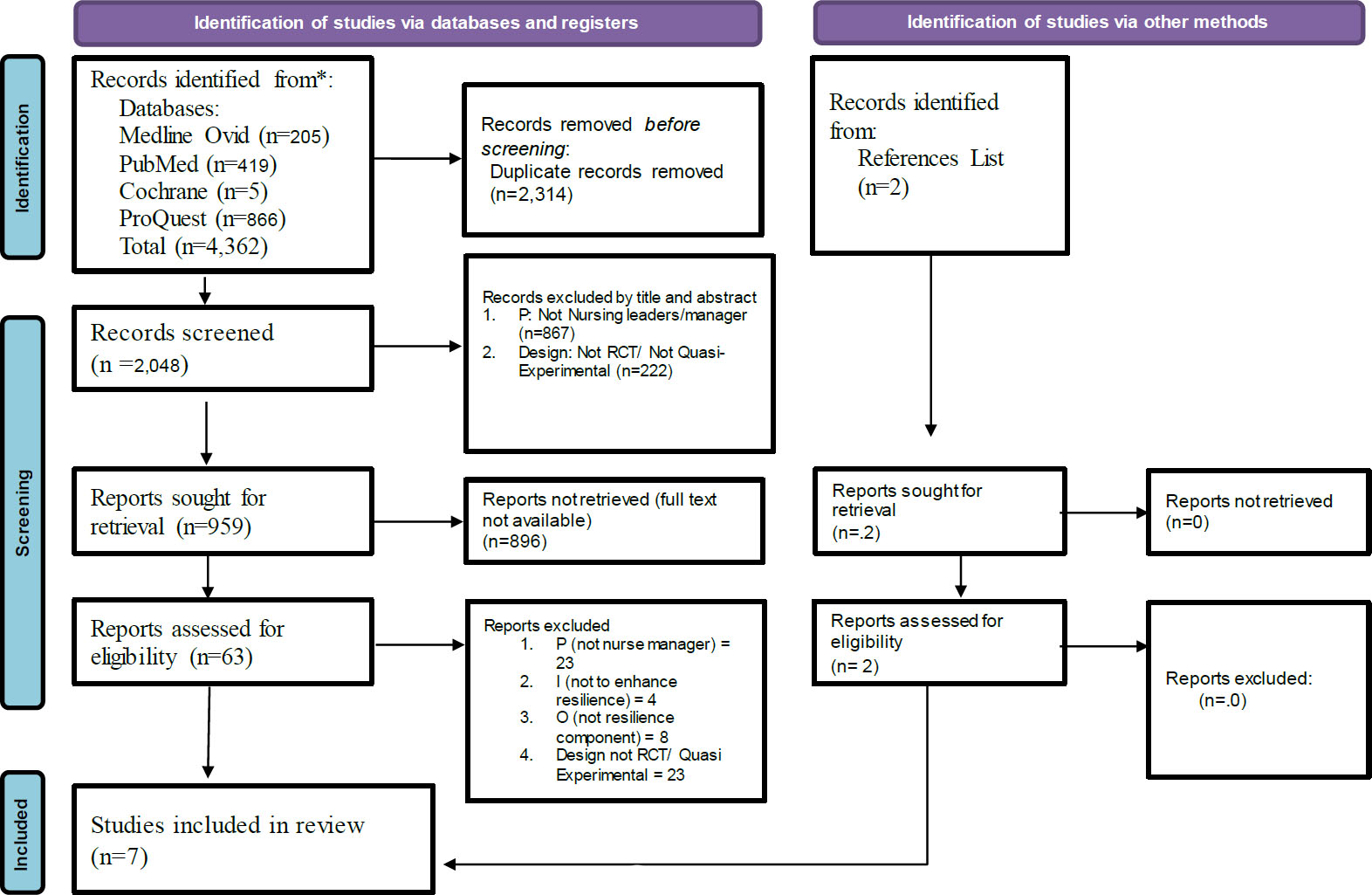
PRISMA flow chart, selection of studies.
across studies, limitations such as inconsistent confidence intervals, small sample sizes, U.S.-centric research, and the exclusion of grey literature reduce global applicability and precision, highlighting the need for broader and more inclusive future research. Coogan and Hampton evaluated a five-session nurse manager orientation program, finding significant improvements in competencies (M = 5.77, SD = 0.720) and psychological empowerment (M = 5.64, SD = 0.655). The study highlights the program's effectiveness in enhancing skills and self-determination in nurse managers [19].
3.3.1. Quality Within Studies
The overall risk of bias across included studies was variable: RCTs were assessed as having a low to moderate risk of bias due to robust randomization methods but limitations in participant and personnel blinding. Meanwhile, Quasi-experimental studies were predominantly rated as having a moderate risk of bias, mainly due to confounding and challenges in classifying interventions.
Figs. (2 and 3) present detailed visual summaries of the bias assessments for RCTs and quasi-experimental studies, respectively. These findings underscore the need for more rigorous design and reporting in future studies to strengthen the evidence base on resilience interventions for nurse managers (Table 1).
4. DISCUSSION
The interventions reviewed varied significantly in structure, content, and delivery methods, making direct comparisons challenging. For example, Alan et al. [13] implemented a web-based crisis management program emphasizing knowledge in crisis management and leadership, while Santos et al. [14] used mindfulness-based interventions to enhance emotional intelligence and resilience. Sawyer et al. [14] introduced a psychoeducational group program addressing resilience, self-compassion, and stress management, whereas Chesak et al. [15] focused on stressors unique to professional mothers through facilitated discussions. Spiva et al. [16] combined self-paced leadership training with resilience coaching, and Shurab et al. [18] developed an authentic leadership and mindfulness program. Lastly, Coogan and Hampton [19] offered a structured nurse manager orientation to improve competencies and empowerment. Despite diverse methods, these interventions demonstrated significant improvements in leadership skills, resilience, and mental well-being, tailored to specific needs and contexts.
The studies highlight the effectiveness of various interventions in improving nurse managers' skills, resilience, leadership, and well-being. Web-based and mindfulness programs were particularly impactful in enhancing knowledge
| No. | Author/Refs. | Country | Design | Sample size | Intervention | Time to Follow up | Outcomes | Instruments | Summary of Key Findings | |
|---|---|---|---|---|---|---|---|---|---|---|
| Experiment | Control | |||||||||
| 1 | Alan et al. (2023) [13] | Turkey | Randomized controlled Experimental Study | 30 | 31 | • Web-Based Crisis Management Training Program • Consist of 9 categories of topics in web-based, each session 35-40 minutes (all modules can be accessed by the intervention group whenever they want) • Duration: 1 month and a half |
Directly after training |
Knowledges, consist of: 1. Management of crises 2. Leadership in crisis 3. Planning and managing Nurse Manpower 4. Supervising and Managing patient Care 5. Logistics and Support Services 6. Communication 7. Motivating Nurse 8. Stress Management 9. Employee Adaptation |
Self-design Likert Scale Questionnaire (points 1-5) with 2-3 questions for each topic of training. A higher score means higher knowledge. | Web-based training programs can effectively improve nurse managers' knowledge levels. The intervention group had a considerably higher mean number of correct post-test responses compared to the control group after the web-based training session (t = 4.982 p < 0.001). |
| 2 | Santos et al. (2024) [14] | Brazil | Randomized crossover clinical trial (a pilot study) | 18 | 14 | • Mindfulness-based intervention, with 12 hours in total • Duration for each session of MBI: 15 minutes |
Post-test: one month after intervention Follow-up: three months after post-test |
• Nurse leaders’ Emotional Intelligence (Sociability, Self-control, Non-Judgement, Act with Awareness) • Nurse Leaders’ resilience | • The Emotional Intelligence Measure • The Connor- Davidson Resilience Questionnaire | The mindfulness-based effectively enhances the emotional intelligence and dispositional mindfulness abilities of nurse leaders. Post-test results The test results showed a statistically significant increase in the emotional intelligence skills of sociability (p=0.009), self-control (p=0.015), and non-judgment (p=0.022) as well as total (p=0.002) mindfulness. Follow-up: The Non-judgment (p=0.024) and Total (p=0.026) mindfulness components showed a noteworthy increase. |
| 3 | Sawyer et al. (2023) [17] | USA | Parallel Randomized controlled trial | 32 | 32 | • Psychoeducational group program • The themes of intervention consist of resilience, insight, self-compassion, and empowerment to fight burnout and enhance purposeful adaptive coping to reduce distress and improve mental well-being. • Duration: nine weekly 90 min group sessions |
One-month follow up Three-month follow-up and six-month follow-up |
• Resilience • Quality of Life • Self-Compassion • Self-Reflection • Self-Efficacy • Perceived Stress • Affective Job Satisfaction |
• Brief Resilience Scale (BRS) • Professional Quality of Life (ProQOL) • Self-Compassion Scale-Short Form (SCS-SF) • Self-Reflection and Insight Scale (SRIS) • General Self-Efficacy Scale (GSE) • Perceived Stress Scale (PSS) • Brief Index of Affective Job Satisfaction (BIAJS) |
The psychoeducational group program can be an effective intervention for improving and protecting mental well-being. The intervention group showed: • No significant difference in resilience from baseline to endpoint (F=0.015, p=0.93). • |
| • There was a significant difference in self-compassion after one month of follow-up (t=-2.82, p=0.008) • Empowerment was significantly higher at the end point than at baseline (t=-2.86, p=0.007). • PSS scores were significantly lower at one month follow-up (t=2.06, p=0.048). |
||||||||||
| 4 | Chesak et al. (2020) [15] | USA | Randomized controlled trial | 18 | 18 | • Authentic Connections Group (AC Groups). • AC Groups intervention consisted of 12 sessions, each lasting one hour. The sessions included facilitated discussions that addressed various stressors faced by professional mothers, such as work-life balance, feelings of shame and self-doubt, and strategies for self-care and support systems. The sessions were designed to be participatory and insight-oriented, fostering a warm and accepting environment for participants. |
Baseline: Before the intervention began. Post-Intervention: Immediately after the completion of the 12-session intervention. Follow-Up: At a later point to assess the sustainability of the intervention's effects. |
The major outcomes measured in the study included: • Depression • Self-compassion • Perceived stress • Anxiety • Emotional exhaustion • Personal accomplishment |
• Zung Self-Rating Depression Scale • Zung Self-Rating Anxiety Scale • Perceived Stress Scale |
• There are significant differences between the intervention and control groups over time for depression, self-compassion, and perceived stress, with large effect sizes (η2p = .20). • Medium effect sizes were observed for increased levels of feeling loved and personal accomplishment (η2p = .07 and .13, respectively), although the former was not statistically significant. • Small to moderate effects were found for decreased anxiety and emotional exhaustion (η2p = .05 and .03). |
| 5 | Spiva et al. (2021) [16] | USA | A quasi-experimental design | 46 | n/a | • Nurse leader training and a • strength-based coaching program • A self-paced online training program for basic nurse manager knowledge and skills. • A single-day workshop for resiliency training • Two coaching sessions separated by 6 months focused on enhancing individually identified strengths. |
Measurement was conducted before the intervention (pre-survey) and after the intervention (post-survey). | The major outcomes • Resiliency • Transformat- ional leadership • Leadership effectiveness • Leadership satisfaction |
• MLQ-5XShort (Multifactor Leadership Questionnaire) for assessing transformational leadership. • CD-RISC-25 (Connor-Davidson Resilience Scale) for measuring resiliency attributes. • Clifton Strengths assessment for identifying individual strengths. |
The intervention was effective in enhancing the transformational leadership skills and resilience of nurse managers: • Resiliency (F = 39.40, p < .001) • Transformat- ional leadership (F = 22.32, p < .001) • Leadership effectiveness (F = 11.89, p = .001) • Leadership satisfaction scores (F = 8.33, p = .006) |
| 6 | Shurab et al. (2024) [18] | Egypt | A quasi-experimental design | 70 | 0 | • Authentic Leadership and Mindfulness Educational Program • 8 sessions, 4 weeks (2 sessions per week), each session lasted 60 minutes |
Immediately after training and 3 months after intervention | • Knowledge • Authentic leadership • Management competencies |
• Authentic Leadership Knowledge questionnaire • Self-reported questionnaire about authentic leadership • The management competencies of nurse manager |
• The results found significant differences (p = 0.001) in nurse managers' knowledge, authentic leadership, mindfulness, and managerial competences before, throughout, and after the three-month program. • Cohen's d test revealed that the educational program had a significant effect on post and follow-up knowledge, authentic leadership, mindfulness, and managerial competency scores (η2=0.6 and 4.58, respectively) |
| 7 | Coogan and Hampton (2020) [19] | USA | A pilot study, pre-post test design | 9 | 0 | • The new nurse manager orientation program • Five sessions completed over an approximate 5-month period |
No Information | • Nurse manager competencies • Psychological empowerment |
• American Organization for Nursing Leadership (AONL) nurse manager competency tool • Spreitzer’s psychological empowerment tool |
Individuals' competence and abilities improve during the intervention • Psychological empowerment (M= 5.64, SD=0.655), self-determination (M=5.08, SD= 0.861) • Individual competencies M= 5.77, SD=0.720) |
and emotional intelligence, while psychoeducational and leadership-focused sessions showed promising results in mental health and leadership competencies. The heterogeneity of these interventions underscores the need for more standardized assessment tools to measure resilience and emotional intelligence objectively.
Cultural and organizational factors also played a significant role in intervention success. Studies conducted in diverse countries highlighted the influence of healthcare systems, workplace norms, and societal expectations on program outcomes [20]. This variability suggests a need for further research on how to adapt these interventions to different cultural and organizational contexts. Additionally, publication bias may have influenced the findings, as the review focused on peer-reviewed studies and may have excluded relevant evidence from grey literature.
Moreover, to improve the practical application of these findings, healthcare organizations should consider tailoring interventions to their specific contexts. Web-based and hybrid training models, such as the Web-based crisis management training program and resolution program, offer cost-effective and scalable solutions [21]. Incorporating mentorship components can further enhance peer support and knowledge transfer. Embedding resilience and leadership training into standard nurse manager development programs can help institutionalize these practices [22]. Policymakers should allocate funding and resources to support these initiatives, particularly in resource-limited settings [23].
4.1. Strengths and Limitations
This systematic review synthesized findings from seven studies aimed at enhancing resilience among nurse managers through various interventions. Three hundred eighteen nurse managers participated in the studies, with most being conducted in the United States and additional contributions from Turkey, Egypt, and Brazil. The interventions included mindfulness-based practices, psychoeducational programs, web-based training, and leadership development initiatives. These programs demonstrated statistically significant improvements in resilience-related outcomes such as stress reduction, emotional intelligence, leadership skills, and mental well-being. These interventions offered valuable resilience-building strategies in high-stress healthcare environments by addressing professional and personal challenges.
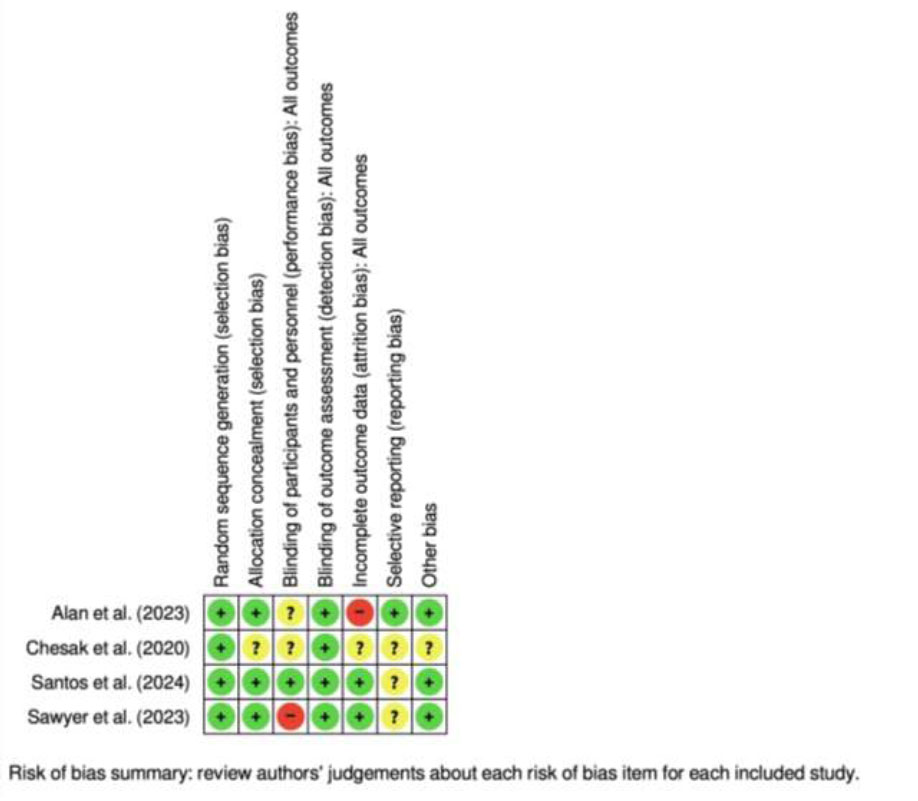
Risk of bias for randomized controlled trials.
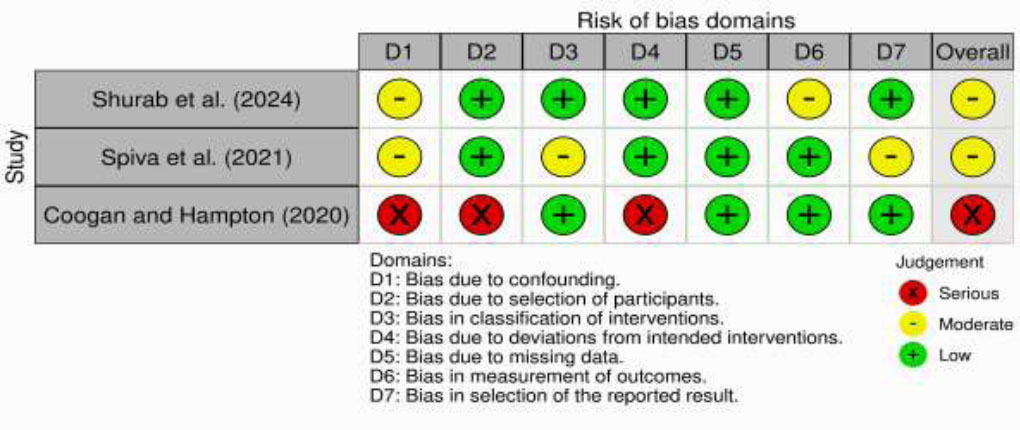
Risk of bias for quasi-experimental study.
Despite these strengths, the studies had notable limitations. Many had small sample sizes (e.g., n=20–85), which reduced statistical power and the ability to generalize findings. Short follow-up periods were standard, capturing immediate or short-term outcomes but leaving long-term effectiveness uncertain. Participant blinding was often unfeasible, introducing potential performance and detection biases. Reliance on self-reported measures for outcomes such as resilience and emotional intelligence further limited the objectivity of the findings. Moreover, the cultural and organizational contexts of the studies varied significantly, and few programs explicitly addressed how these factors influenced their success. It limits their adaptability to diverse healthcare settings.
4.2. Future Research
Future research should address the methodological limitations of existing studies by using larger sample sizes, extending follow-up periods, and adopting multi-site study designs. Developing and validating standardized tools for measuring resilience and emotional intelligence will improve the reliability of findings. Studies should also explore the impact of cultural, gender, and generational differences on intervention effectiveness. Additionally, research should assess the organizational impact of improved resilience among nurse managers, including effects on team dynamics, staff retention, and patient care quality.
This review highlights the significant potential of tailored, evidence-based interventions to enhance resilience and leadership among nurse managers. Addressing methodological limitations, cultural variability, and long-term effectiveness will be crucial for broader implementation. By integrating these interventions into organizational strategies and policy frameworks, healthcare systems can better equip nurse managers to thrive in high-pressure environments, benefiting their teams and patients.
CONCLUSION
Resilience-building interventions for nurse managers are a valuable strategy for enhancing leadership, reducing burnout, and improving team performance. Healthcare organizations should consider integrating multifaceted approaches that address emotional intelligence and leadership development to support their nurse leaders effectively. Future research should continue to refine these interventions and explore their long-term impact on resilience and organizational outcomes, focusing on technology, cross-cultural adaptation, and standardized measurement tools to strengthen the evidence base for resilience-building strategies in healthcare leadership. Future research on resilience-building interventions for nurse managers should focus on several key areas. Studies should explore the use of digital platforms, such as mobile apps and online modules, to make interventions more accessible and scalable. Cross-cultural adaptations are necessary to tailor interventions to diverse healthcare settings and leadership styles. Developing standardized tools to measure resilience and leadership outcomes will enhance comparability and provide reliable data. Additionally, long-term studies are needed to assess the sustainability of these interventions and their impact on organizational outcomes, such as nurse retention, job satisfaction, and patient care quality, demonstrating their broader value.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: H.M.: Study conception and design; R.S.: Data collection; Y.P.L., C.Y.L.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| PPE | = Personal Protective Equipment |
| RCTs | = Randomized Controlled Trials |
| ROBINS-I | = Risk of Bias in Non-Randomized Studies of Interventions |
ETHICAL STATEMENT
The research committee is Faculty of Nursing, Universitas Andalas, with reference number: 106.laiketik/KEPPKFKEPUNAND.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Repository of Universitas Andalas at http://repo.unand.ac.id/id/eprint/51747 (reference number 51747).
FUNDING
This study has been granted funding from Higher Education, Research and Community Service, Ministry of Education, Research and Technology of Indonesia, Indonesia Government, number: 0459/E5/PG.02.00/2024 30 Mei 2024
ACKNOWLEDGEMENTS
Declared none.